Abdominal Wall Defects
An abdominal wall defect is a birth defect in which the digestive organs, such as the stomach or intestines, push out of the body through an abnormal opening in the baby’s belly (abdomen). Abdominal wall defects are rare and occur in approximately 2 to 2.5 out of every 10,000 live births.
About Abdominal Wall Defects
At around 6 weeks of gestation, the folds in tissue that form the front abdominal wall of the fetus may not close completely, resulting in an opening or defect. This defect can vary in size and location. If the upper fold of the abdominal tissue does not close, the defect is located near the bottom of the breastbone (sternum) of the baby, which may be associated with a pentalogy of Cantrell anomaly. If the side folds of the abdominal wall do not close, a mid-abdomen defect (omphalocele) occurs. If the lower fold of the abdominal wall does not close, then the defect is in the area near the bladder (bladder exstrophy) and can result in the bladder being located outside of the abdomen.
Types of abdominal wall defects include:
- Bladder exstrophy occurs in approximately 1 out of every 10,000 live births. When the abdominal wall defect is very low, the bladder opens to the skin just above the pubic bone.
- Body stalk abnormality occurs in approximately 1 out of every 7,500 live fetuses. This is the most severe form of an abdominal wall defect in which the wall of the abdomen never really forms and the baby appears “stuck” to the placenta. As a result, the umbilical cord is very short and there is no amniotic fluid surrounding the fetus.
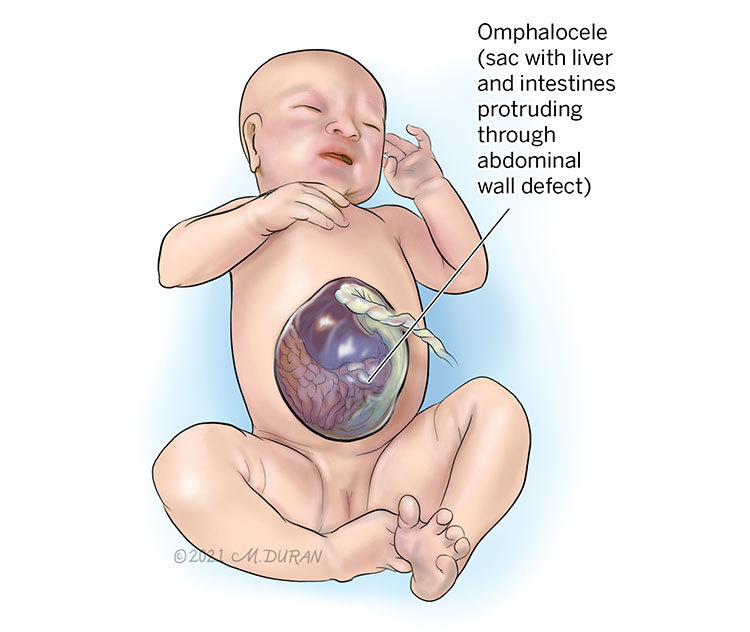
- Omphalocele occurs in approximately 1 out of every 7,000 live births. This central defect in the abdomen, just under the umbilical cord area, results in a sac, containing the liver and sometimes the intestines, that protrudes from the abdomen with the umbilical cord now located at the top part of the sac.
- Pentalogy of Cantrell occurs in approximately 1 out of every 65,000 to 200,000 live births. This midline birth defect usually involves five different problems in babies, which include a heart defect, a missing section of the covering of the heart (pericardium), a missing lower part of the breastbone (sternum), a missing part of the diaphragm (the muscle tissue that separates the lungs from the organs in the abdomen), and an upper defect in the abdominal wall. Although some babies might not have all five problems, they may still be given the diagnosis of pentalogy of Cantrell.
Causes of Abdominal Wall Defects
The cause of abdominal wall defects remains unknown, and there are no known genetic mutations associated with the cause of this condition.
Complications Associated With Abdominal Wall Defects
Fetal abdominal wall defects are rarely associated with any health risks for the pregnant mother. However, complications with other organs in a fetus with an abdominal wall defect are very common. Omphaloceles that are large in size are associated with poor development of the lungs (pulmonary hypoplasia). Some fetuses with an abdominal wall defect may also develop problems with a slowing of their growth known as intrauterine growth restriction. The reason for this is unclear. A fetus with an abdominal wall defect is at an increased risk for dying in the womb. Chromosomal abnormalities in fetuses with abdominal wall defects are also very common. Omphaloceles that are small in size and do not contain the liver appear to be at higher risk for chromosomal abnormalities. Some abdominal wall defects are associated with genetic syndromes (a collections of physical findings that are given a specific name).
The long-term outcome for babies with abdominal wall defects is dependent on the size of the defect, whether other organs, such as the heart, are abnormal and whether the cause of the defect is a chromosomal problem or a genetic syndrome.
Diagnosing Abdominal Wall Defects
Sometimes, the pregnant mother will undergo a blood test known as an alpha-fetoprotein (AFA) test. This is usually performed to detect spina bifida in the fetus; however, elevated levels of alpha-fetoprotein can also be associated with abdominal wall defects. Abdominal wall defects are more commonly found at the time of an anatomy ultrasound at around 20 weeks (5 months) of gestation. A protruding mass, containing intestines and the liver, appears on the front side of the fetus, and the umbilical cord is located at the very top of the mass of an omphalocele.
Pregnancy With Abdominal Wall Defects
After the initial ultrasound evaluation, you will likely be scheduled for a fetal echocardiogram (specialized ultrasound of the heart) to assess for congenital heart disease and fetal magnetic resonance imaging (MRI) to assess the other organ systems in the fetus. A fetal MRI is similar to a CT scan but does not involve X-rays or radiation. Instead, a special magnet is used to produce images of the structures in the fetus that cannot be seen easily with ultrasound. A fetal MRI is safe for both you and your baby. You will be scheduled to meet with a genetic counselor to discuss your baby’s risk for developing chromosomal problems as well as the available tests that can be completed during your pregnancy to identify these types of problems. During your pregnancy, you may also be scheduled to meet with a pediatric surgeon depending on whether the defect can be fixed with surgery. If there is evidence of heart problems in the fetus, you will be scheduled to meet with a pediatric cardiologist and a pediatric cardiovascular surgeon.
You will be scheduled for ultrasounds every 3 to 4 weeks to monitor your baby’s rate of growth. At around 32 weeks (8 months) of gestation, you will be scheduled weekly for a biophysical profile. This is an ultrasound test that measures the amount of fluid around the baby as well as how the baby is moving and breathing. The biophysical profile testing may be started before 32 weeks of gestation if problems with the growth of the baby arise. You may also be asked to do a fetal kick count assessment, where you count the number of times your baby moves each night to keep a record.
Typically, most women with a baby in utero with an abdominal wall defect will be induced at around 37 weeks (3 weeks before your due date) of gestation. You may be scheduled to deliver earlier if an ultrasound reveals that the fetus has stopped growing in the womb, the biophysical profile testing reveals the fetus is in distress, or if you report decreased fetal movement. A vaginal delivery is safe for fetuses with an abdominal wall defect that is small in size (less than 5 cm in diameter), but delivery be C-section may be necessary. Omphaloceles that are larger in size (greater than 5 cm in diameter) or contain the liver are usually delivered by C-section to keep the sac from tearing at birth.
Treating Abdominal Wall Defects
There are currently no forms of fetal surgery available for treating abdominal wall defects. All treatments are performed after your baby is born.
Evaluation After Birth
After birth, your baby will be wrapped in a sterile wet towel and transported to the neonatal intensive care unit (NICU). A pediatric surgeon will evaluate the baby soon after they are born to decide what form of surgery may be needed and when the operation should occur. In some cases, an omphalocele is treated with antibiotic creams so that the skin will continue to grow up on the sides. Your baby may be sent home with you to continue this treatment, and later, after the baby has further developed, your pediatric surgeons may schedule your baby for surgery to fix the defect.
Care Team Approach
The Comprehensive Fetal Care Center, a clinical partnership between Dell Children's Medical Center and UT Health Austin, takes a multidisciplinary approach to your child’s care. This means you and your child will benefit from the expertise of multiple specialists across a variety of disciplines. Your care team will include fetal medicine specialists, obstetricians, neonatologists, sonographers, palliative care providers, fetal center advanced practice providers, fetal center nurse coordinators, genetic counselors, and more, who work together to provide unparalleled care for patients every step of the way. We collaborate with our colleagues at The University of Texas at Austin and the Dell Medical School to utilize the latest research, diagnostic, and treatment techniques, allowing us to identify new therapies to improve treatment outcomes. We are committed to communicating and coordinating your care with your other healthcare providers to ensure that we are providing you with comprehensive, whole-person care.
Learn More About Your Care Team

Comprehensive Fetal Care Center
Dell Children's Specialty Pavilion
4910 Mueller Blvd. Austin, TX 78723
1-512-324-0040
Get Directions